Pharmacotherapeutic Group: Taxanes.
ATC Code: L01CD02.
Pharmacology: Pharmacodynamics: Preclinical data: Docetaxel is an antineoplastic agent which acts by promoting the assembly of tubulin into stable microtubules and inhibits their disassembly which leads to a marked decrease of free tubulin. The binding of docetaxel to microtubules does not alter the number of protofilaments.
Docetaxel has been shown in vitro to disrupt the microtubular network in cells which is essential for vital mitotic and interphase cellular functions.
Docetaxel was found to be cytotoxic in vitro against various murine and human tumour cell lines and against freshly excised human tumour cells in clonogenic assays. Docetaxel achieves high intracellular concentrations with a long cell residence time. In addition, docetaxel was found to be active on some but not all cell lines over expressing the p-glycoprotein which is encoded by the multidrug resistance gene. In vivo, docetaxel is schedule independent and has a broad spectrum of experimental antitumour activity against advanced murine and human grafted tumours.
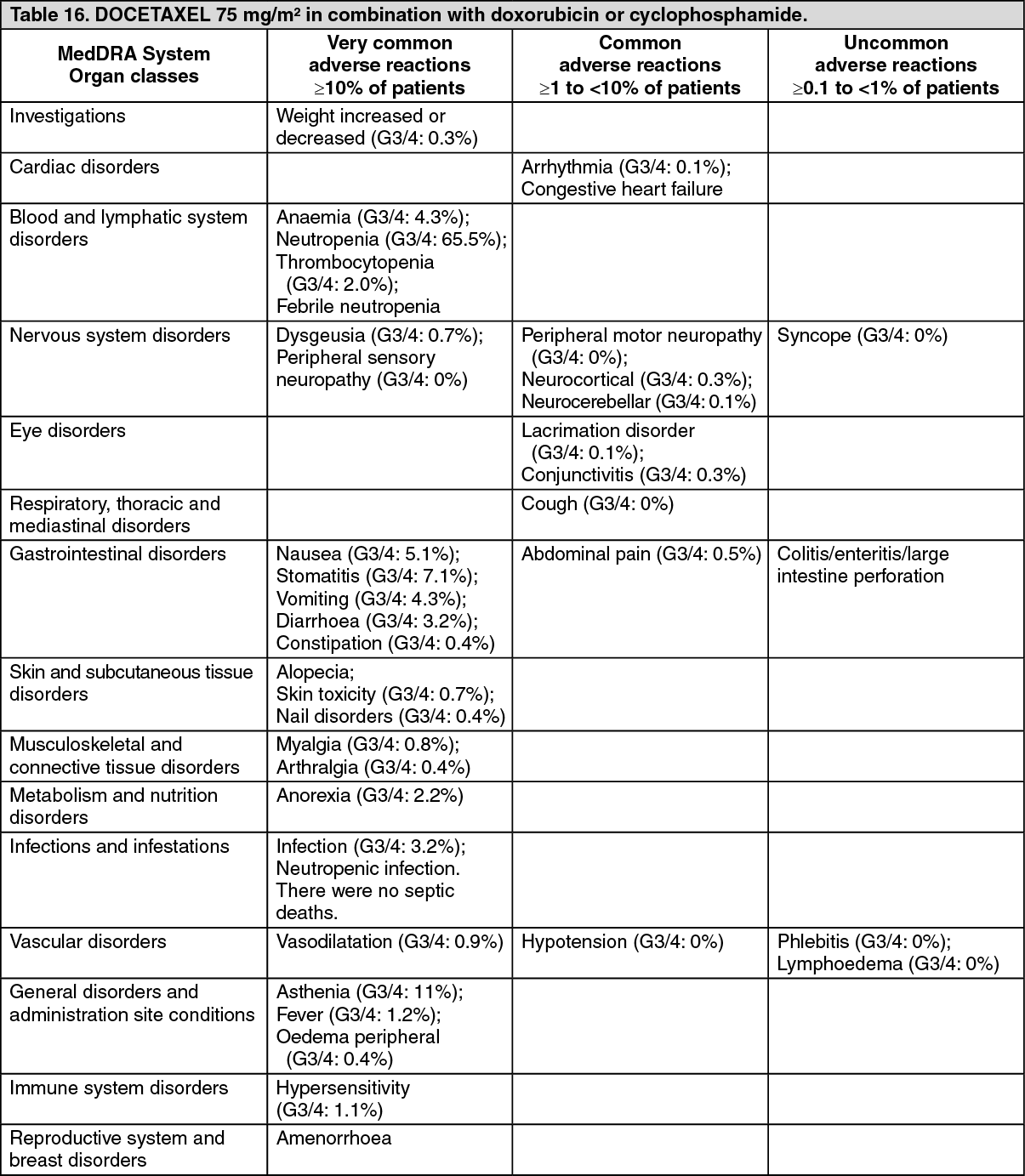
Clinical data: Breast cancer: DOCETAXEL in combination with doxorubicin and cyclophosphamide: adjuvant therapy: Data from a multicenter open label randomized trial support the use of docetaxel for the adjuvant treatment of patients with operable node-positive breast cancer and KPS ≥ 80%, between 18 and 70 years of age. After stratification according to the number of positive lymph nodes (1-3, 4+), 1491 patients were randomized to receive either docetaxel 75 mg/m
2 administered 1-hour after doxorubicin 50 mg/m
2 and cyclophosphamide 500 mg/m
2 (TAC arm), or doxorubicin 50 mg/m
2 followed by fluorouracil 500 mg/m
2 and cyclophosphamide 500 mg/m
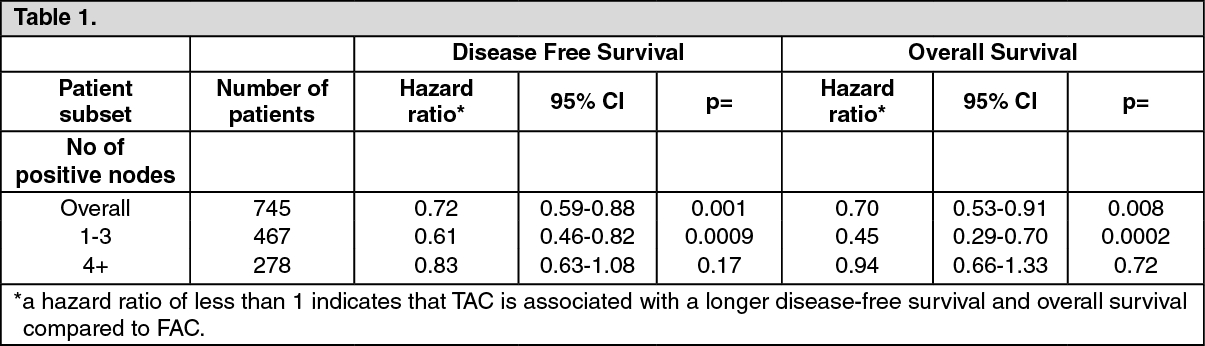
2 (FAC arm). Both regimens were administered once every 3 weeks for 6 cycles. Docetaxel was administered as a 1-hour infusion, all other medicinal products were given as intravenous bolus on day one. G-CSF was administered as secondary prophylaxis to patients who experienced complicated neutropenia (febrile neutropenia, prolonged neutropenia, or infection). Patients on the TAC arm received antibiotic prophylaxis with ciprofloxacin 500 mg orally twice daily for 10 days starting on day 5 of each cycle, or equivalent. In both arms, after the last cycle of chemotherapy, patients with positive estrogen and/or progesterone receptors received tamoxifen 20 mg daily for up to 5 years. Adjuvant radiation therapy was prescribed according to guidelines in place at participating institutions and was given to 69% of patients who received TAC and 72% of patients who received FAC. An interim analysis was performed with a median follow up of 55 months. Significantly longer disease-free survival for the TAC arm compared to the FAC arm was demonstrated. Incidence of relapses at 5 years was reduced in patients receiving TAC compared to those who received FAC (25% versus 32%, respectively) i.e. an absolute risk reduction by 7% (p = 0.001). Overall survival at 5 years was also significantly increased with TAC compared to FAC (87% versus 81%, respectively) i.e. an absolute reduction of the risk of death by 6% (p = 0.008). TAC-treated patient subsets according to prospectively defined major prognostic factors were analyzed: see Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The beneficial effect of TAC was not proven in patients with 4 and more positive nodes (37% of the population) at the interim analysis stage. The effect appears to be less pronounced than in patients with 1-3 positive nodes. The benefit/risk ratio was not defined fully in patients with 4 and more positive nodes at this analysis stage.
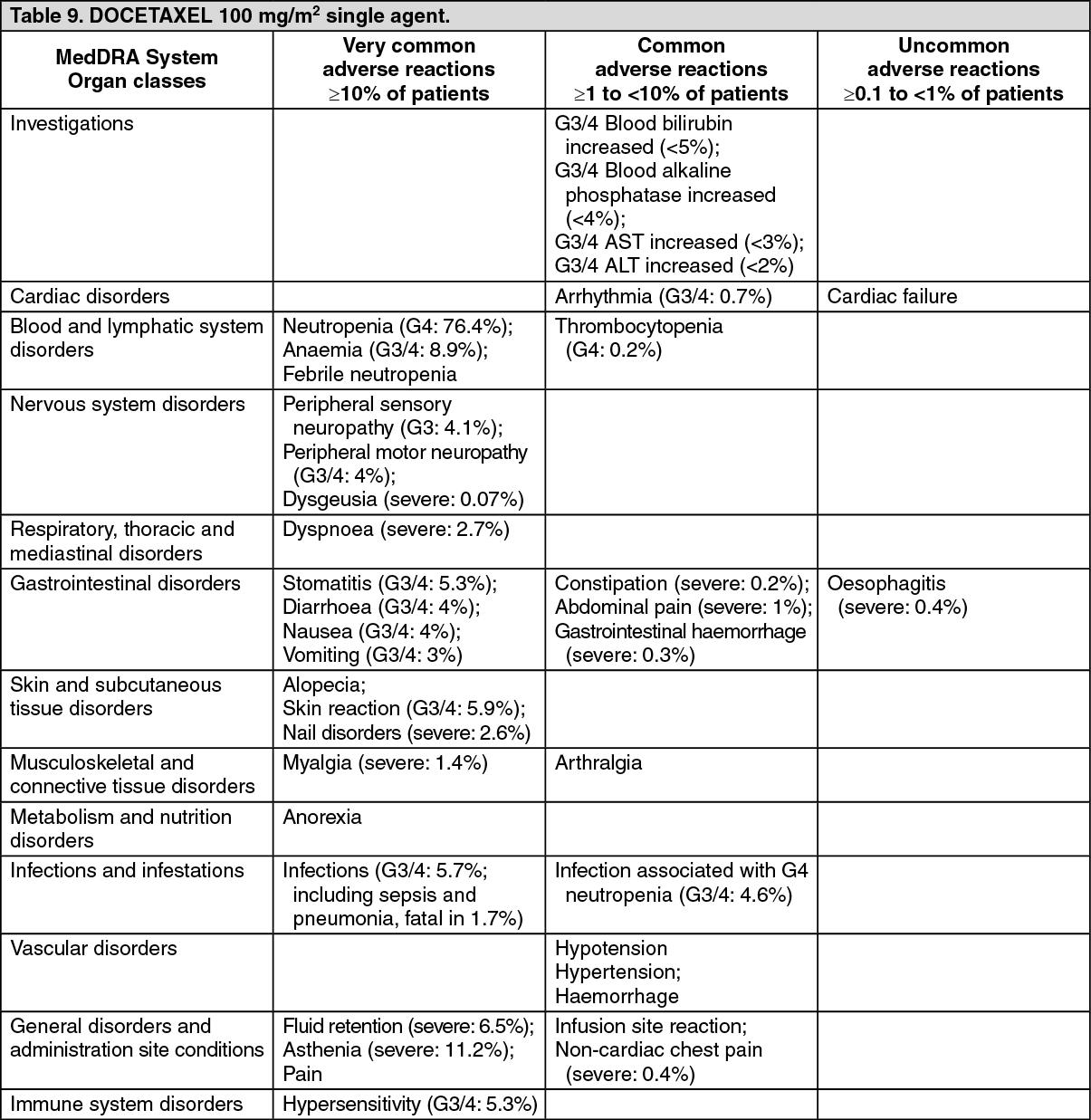
DOCETAXEL as single agent: Two randomised phase III comparative studies, involving a total of 326 alkylating or 392 anthracycline failure metastatic breast cancer patients, have been performed with docetaxel at the recommended dose and regimen at 100 mg/m
2 every 3 weeks.
In alkylating-failure patients, docetaxel was compared to doxorubicin (75 mg/m
2 every 3 weeks). Without affecting overall survival time (docetaxel 15 months vs. doxorubicin 14 months, p = 0.38) or time to progression (docetaxel 27 weeks vs. doxorubicin 23 weeks, p = 0.54), docetaxel increased response rate (52% vs. 37%, p = 0.01) and shortened time to response (12 weeks vs. 23 weeks, p = 0.007). Three docetaxel patients (2%) discontinued the treatment due to fluid retention, whereas 15 doxorubicin patients (9%) discontinued due to cardiac toxicity (three cases of fatal congestive heart failure).
In anthracycline-failure patients, docetaxel was compared to the combination of mitomycin C and vinblastine (12 mg/m
2 every 6 weeks and 6 mg/m
2 every 3 weeks). Docetaxel increased response rate (33% vs. 12%, p < 0.0001), prolonged time to progression (19 weeks vs. 11 weeks, p = 0.0004) and prolonged overall survival (11 months vs. 9 months, p = 0.01).
During these two phase III studies, the safety profile of docetaxel was consistent with the safety profile observed in phase II studies (see Adverse Reactions).
An open-label, multicenter, randomized phase III study was conducted to compare docetaxel monotherapy and paclitaxel in the treatment of advanced breast cancer in patients whose previous therapy should have included an anthracycline. A total of 449 patients were randomized to receive either docetaxel monotherapy 100 mg/m
2 as a 1 hour infusion or randomized to receive either docetaxel monotherapy 100 mg/m
2 as a 1 hour infusion or paclitaxel 175 mg/m
2 as a 3 hour infusion. Both regimens were administered every 3 weeks.
Without affecting the primary endpoint, overall response rate (32% vs 25%, p = 0.10), docetaxel prolonged median time to progression (24.6 weeks vs 15.6 weeks; p < 0.01) and median survival (15.3 months vs 12.7 months; p = 0.03).
More grade 3/4 adverse events were observed for docetaxel monotherapy (55.4%) compared to paclitaxel (23.0%).
DOCETAXEL in combination with doxorubicin: One large randomized phase III study, involving 429 previously untreated patients with metastatic disease, has been performed with doxorubicin (50 mg/m
2) in combination with docetaxel (75 mg/m
2) (AT arm) versus doxorubicin (60 mg/m
2) in combination with cyclophosphamide (600 mg/m
2) (AC arm). Both regimens were administered on day 1 every 3 weeks.
Time to progression (TTP) was significantly longer in the AT arm versus AC arm, p = 0.0138. The median TTP was 37.3 weeks (95% CI: 33.4 - 42.1) in AT arm and 31.9 weeks (95% CI: 27.4 - 36.0) in AC arm.
Overall response rate (ORR) was significantly higher in the AT arm versus AC arm, p = 0.009. The ORR was 59.3% (95% CI: 52.8 - 65.9) in AT arm versus 46.5% (95% CI: 39.8 - 53.2) in AC arm.
In this trial, AT arm showed a higher incidence of severe neutropenia (90% versus 68.6%), febrile neutropenia (33.3% versus 10%), infection (8% versus 2.4%), diarrhea (7.5% versus 1.4%), asthenia (8.5% versus 2.4%), and pain (2.8% versus 0%) than AC arm. On the other hand, AC arm showed a higher incidence of severe anemia (15.8% versus 8.5%) than AT arm, and in addition, a higher incidence of severe cardiac toxicity: congestive heart failure (3.8% versus 2.8%), absolute LVEF decrease ≥20% (13.1% versus 6.1%), absolute LVEF decrease ≥30% (6.2% versus 1.1%). Toxic deaths occurred in 1 patient in the AT arm (congestive heart failure) and in 4 patients in the AC arm (1 due to septic shock and 3 due to congestive heart failure).
In both arms, quality of life measured by the EORTC questionnaire was comparable and stable during treatment and follow-up.
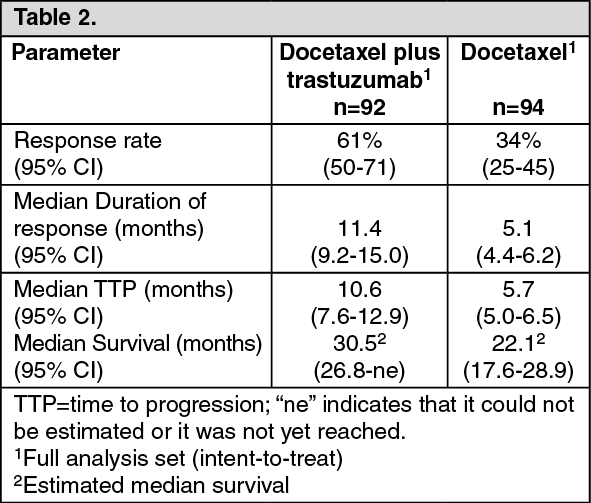
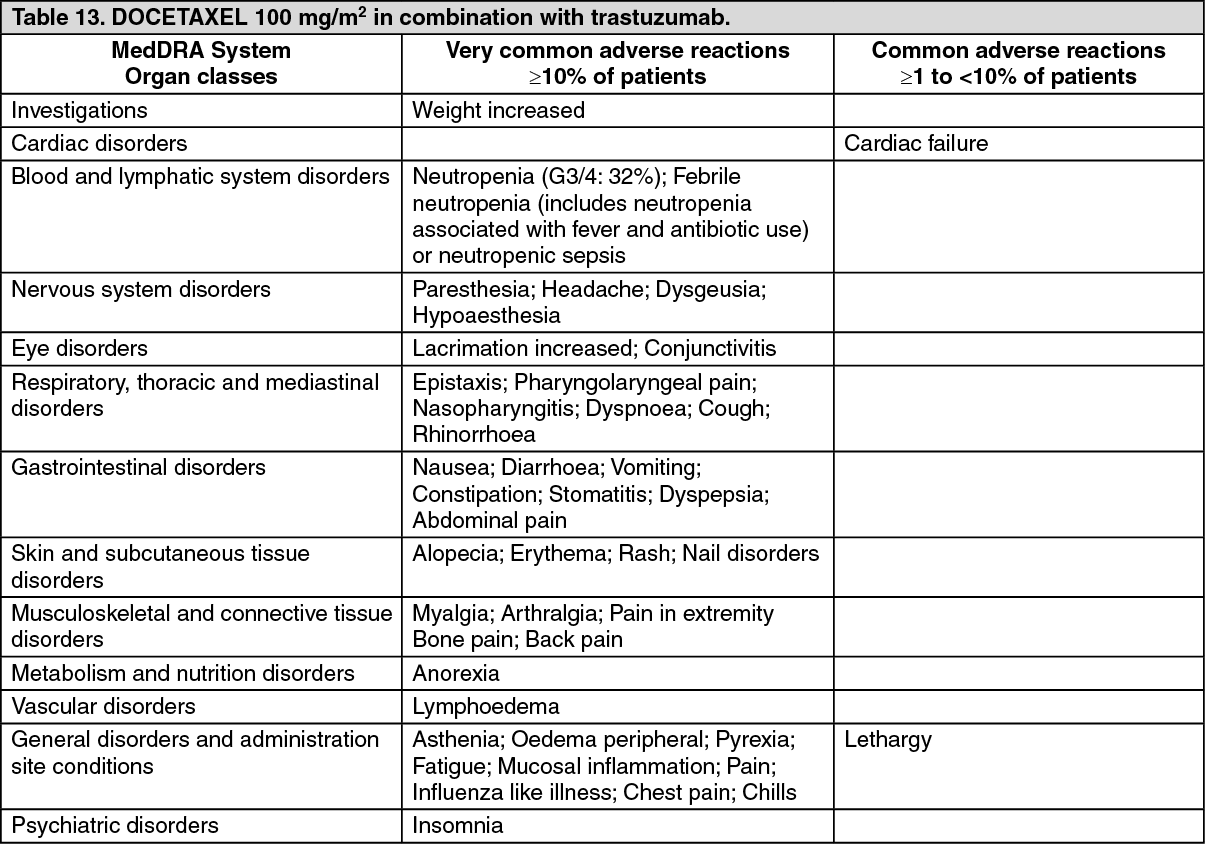
DOCETAXEL in combination with trastuzumab: Docetaxel in combination with trastuzumab was studied for the treatment of patients with metastatic breast cancer whose tumors overexpress HER2, and who previously had not received chemotherapy for metastatic disease. One hundred eighty six patients were randomized to receive docetaxel (100 mg/m
2) with or without trastuzumab; 60% of patients received prior anthracycline-based adjuvant chemotherapy. Docetaxel plus trastuzumab was efficacious in patients whether or not they had received prior adjuvant anthracyclines. The main test method used to determine HER2 positivity in this pivotal trial was immunohistochemistry (IHC). A minority of patients were tested using fluorescence in-situ hybridization (FISH). In this trial, 87% of patients had disease that was IHC 3+, and 95% of patients entered had disease that was IHC 3+ and/or FISH positive, Efficacy results are summarized in the following table: see Table 2.
Click on icon to see table/diagram/image
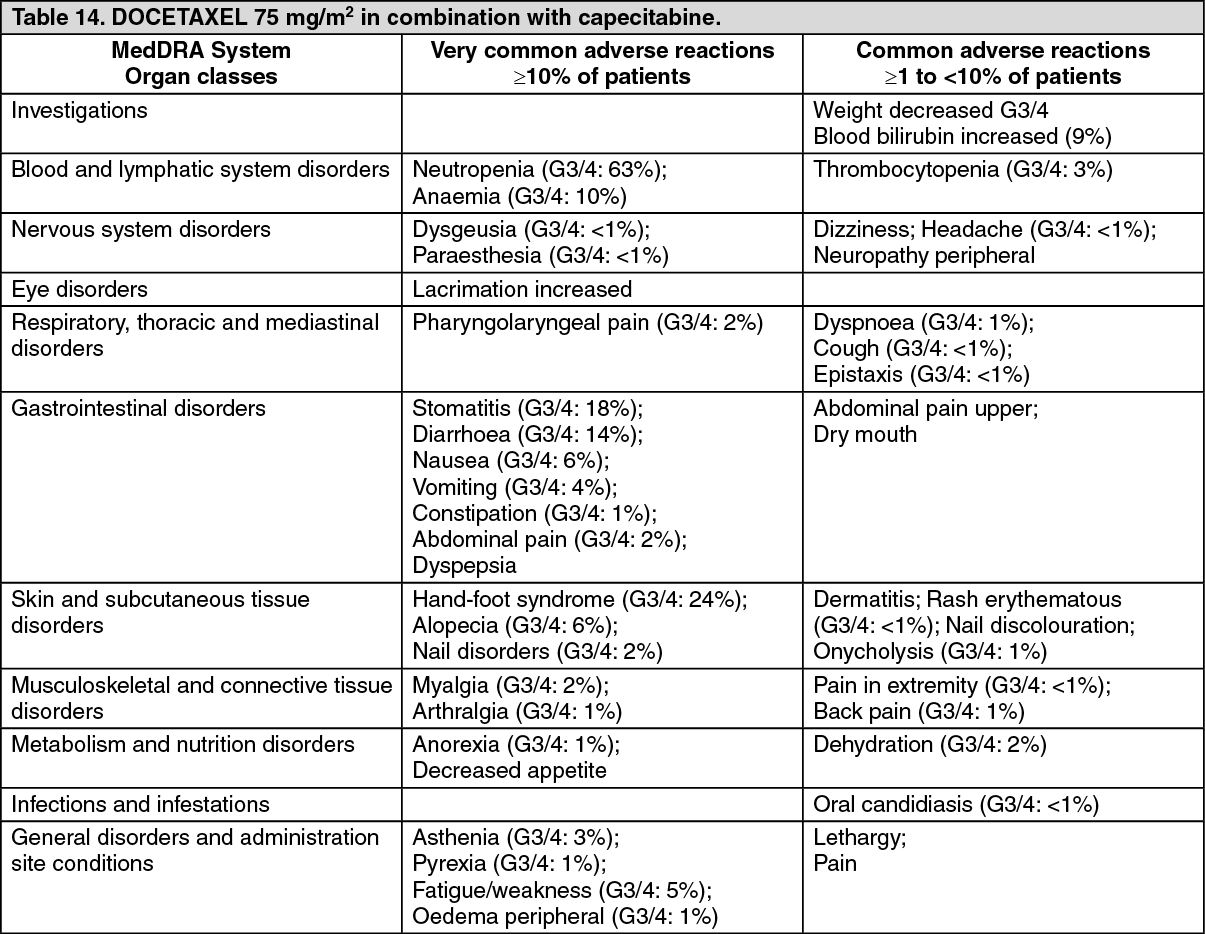
DOCETAXEL in combination with capecitabine: Data from one multicenter, randomised, controlled phase III clinical trial support the use of docetaxel in combination with capecitabine for treatment of patients with locally advanced or metastatic breast cancer after failure of cytotoxic chemotherapy, including an anthracycline. In this trial, 255 patients were randomised to treatment with docetaxel (75 mg/m
2 as a 1 hour intravenous infusion every 3 weeks) and capecitabine (1250 mg/m
2 twice daily for 2 weeks followed by 1-week rest period). 256 patients were randomised to treatment with docetaxel alone (100 mg/m
2 as a 1 hour intravenous infusion every 3 weeks). Survival was superior in the docetaxel + capecitabine combination arm (p = 0.0126). Median survival was 442 days (docetaxel + capecitabine) vs. 352 days (docetaxel alone). The overall objective response rates in the all-randomised population (investigator assessment) were 41.6% (docetaxel + capecitabine) vs. 29.7% (docetaxel alone); p = 0.0058. Time to progressive disease was superior in the docetaxel + capecitabine combination arm (p < 0.0001). The median time to progression was 186 days (docetaxel + capecitabine) vs. 128 days (docetaxel alone).
Non-small cell lung cancer: Patients previously treated with chemotherapy with or without radiotherapy: In a phase III study, in previously treated patients, time to progression (12.3 weeks versus 7 weeks) and overall survival were significantly longer for docetaxel at 75 mg/m
2 compared to Best Supportive Care. The 1-year survival rate was also significantly longer in docetaxel (40%) versus BSC (16%). There was less use of morphinic analgesic (p < 0.01), non-morphinic analgesics (p < 0.01), other disease-related medications (p = 0.06) and radiotherapy (p < 0.01) in patients treated with docetaxel at 75 mg/m
2 compared to those with BSC. The overall response rate was 6.8% in the evaluable patients, and the median duration of response was 26.1 weeks.
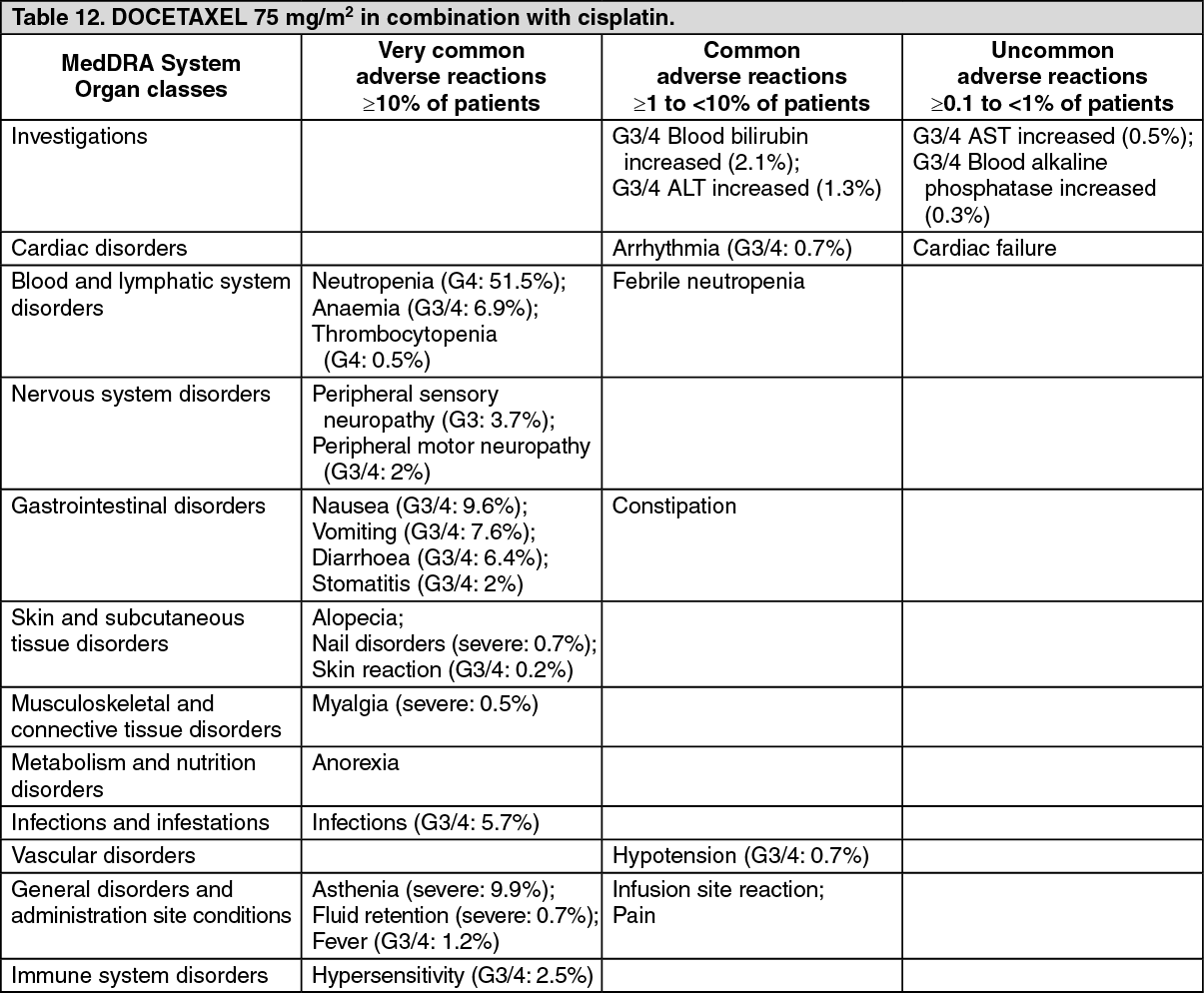
DOCETAXEL in combination with platinum agents in chemotherapy-naïve patients: In a phase III trial, 1218 patients with unresectable stage IIIB or IV NSCLC, with KPS of 70% or greater, and who did not receive previous chemotherapy for this condition, were randomised to either docetaxel (T) 75 mg/m
2 as a 1 hour infusion immediately followed by cisplatin (Cis) 75 mg/m
2 over 30-60 minutes every 3 weeks, docetaxel 75 mg/m
2 as a 1 hour infusion in combination with carboplatin (AUC 6 mg/ml·min) over 30-60 minutes every 3 weeks, or vinorelbine (V) 25 mg/m
2 administered over 6-10 minutes on days 1, 8, 15, 22 followed by cisplatin 100 mg/m
2 administered on day 1 of cycles repeated every 4 weeks.
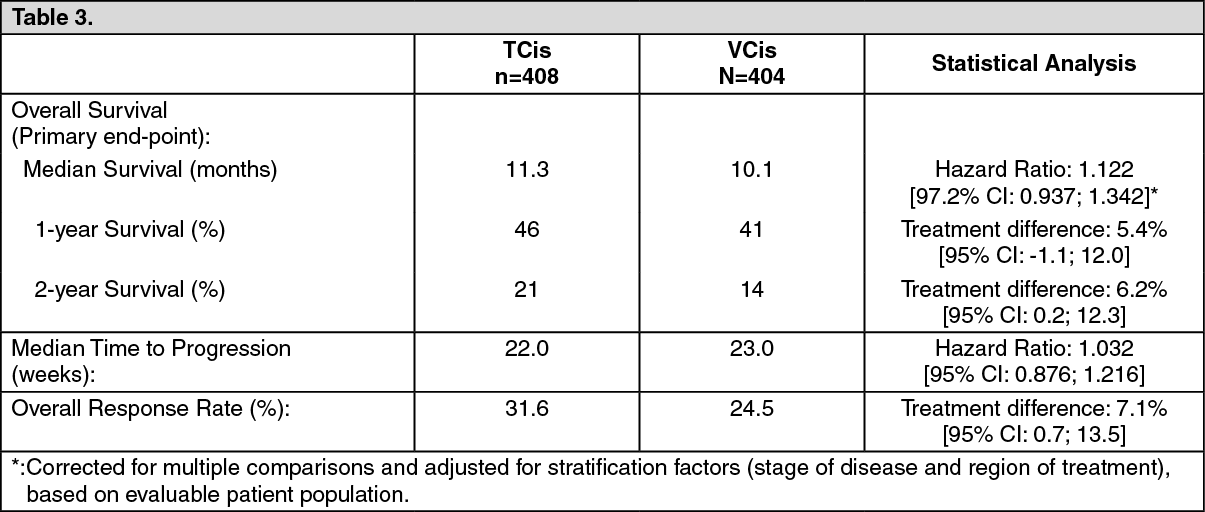
Survival data, median time to progression and response rates for two arms of the study are illustrated in the following table: see Table 3.
Click on icon to see table/diagram/image
Secondary end-points included change of pain, global rating of quality of life by EuroQoL-5D, Lung Cancer Symptom Scale, and changes in Karnofsky performance status. Results on these end-points were supportive of the primary end-points results.
For docetaxel/carboplatin combination, neither equivalent nor non-inferior efficacy could be proven compared to the reference treatment combination VCis.
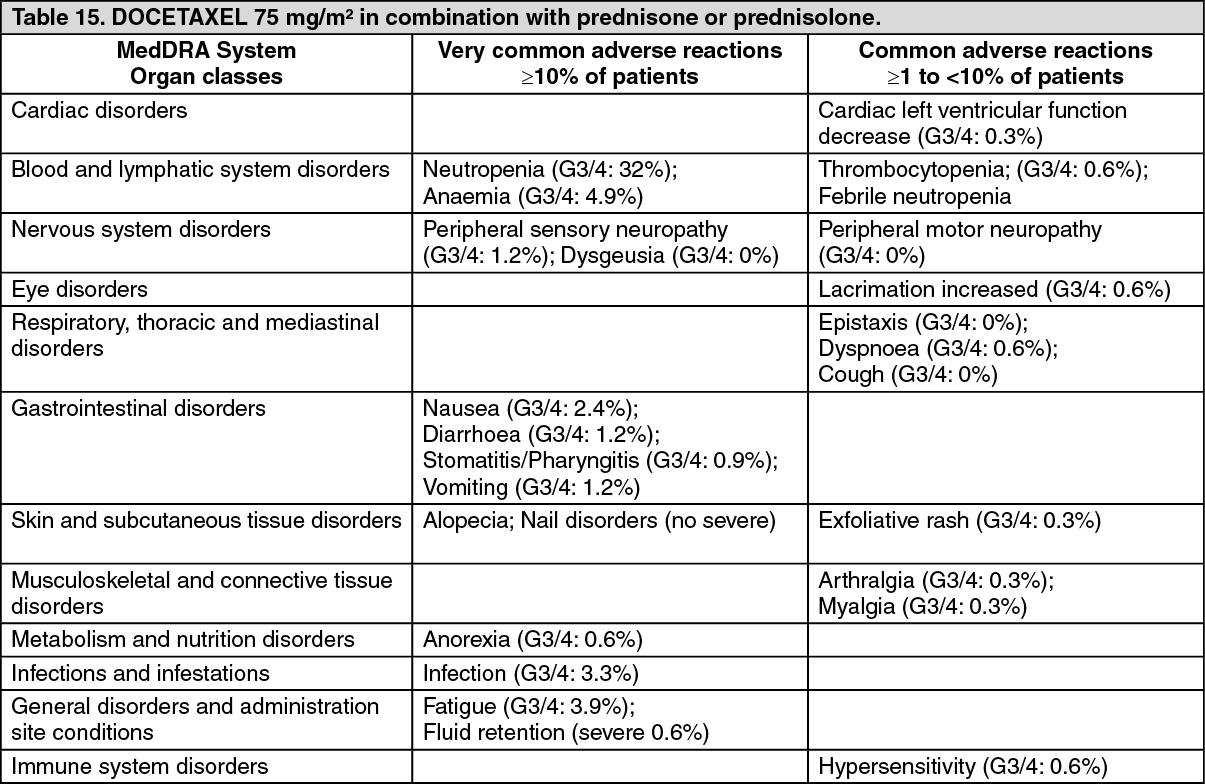
Prostate cancer: The safety and efficacy of docetaxel in combination with prednisone or prednisolone in patients with hormone refractory metastatic prostate cancer were evaluated in a randomized multicenter phase III trial. A total of 1006 patients with KPS ≥ 60 were randomized to the following treatment groups: Docetaxel 75 mg/m
2 every 3 weeks for 10 cycles; Docetaxel 30 mg/m
2 administered weekly for the first 5 weeks in a 6 week cycle for 5 cycles; Mitoxantrone 12 mg/m
2 every 3 weeks for 10 cycles.
All 3 regimens were administered in combination with prednisone or prednisolone 5 mg twice daily, continuously.
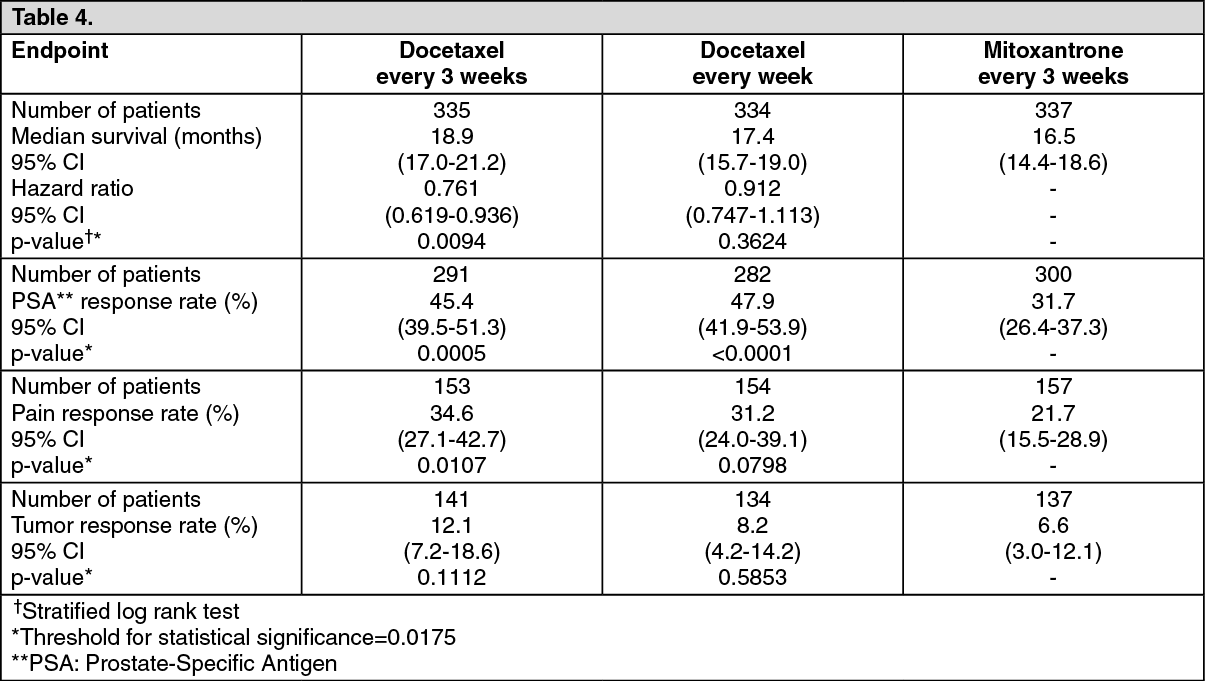
Patients who received docetaxel every three weeks demonstrated significantly longer overall survival compared to those treated with mitoxantrone. The increase in survival seen in the docetaxel weekly arm was not statistically significant compared to the mitoxantrone control arm. Efficacy endpoints for the docetaxel arms versus the control arm are summarized in the following table: see Table 4.
Click on icon to see table/diagram/image
Given the fact that docetaxel every week presented a slightly better safety profile than docetaxel every 3 weeks, it is possible that certain patients may benefit from docetaxel every week. No statistical differences were observed between treatment groups for Global Quality of Life.
Gastric adenocarcinoma: A multicenter, open-label, randomized trial, was conducted to evaluate the safety and efficacy of docetaxel for the treatment of patients with metastatic gastric adenocarcinoma, including adenocarcinoma of the gastroesophageal junction, who had not received prior chemotherapy for metastatic disease. A total of 445 patients with KPS > 70 were treated with either docetaxel (T) (75 mg/m
2 on day 1) in combination with cisplatin (C) (75 mg/m
2 on day 1) and 5-fluorouracil (F) (750 mg/m
2 per day for 5 days) or cisplatin (100 mg/m
2 on day 1) and 5-fluorouracil (1000 mg/m
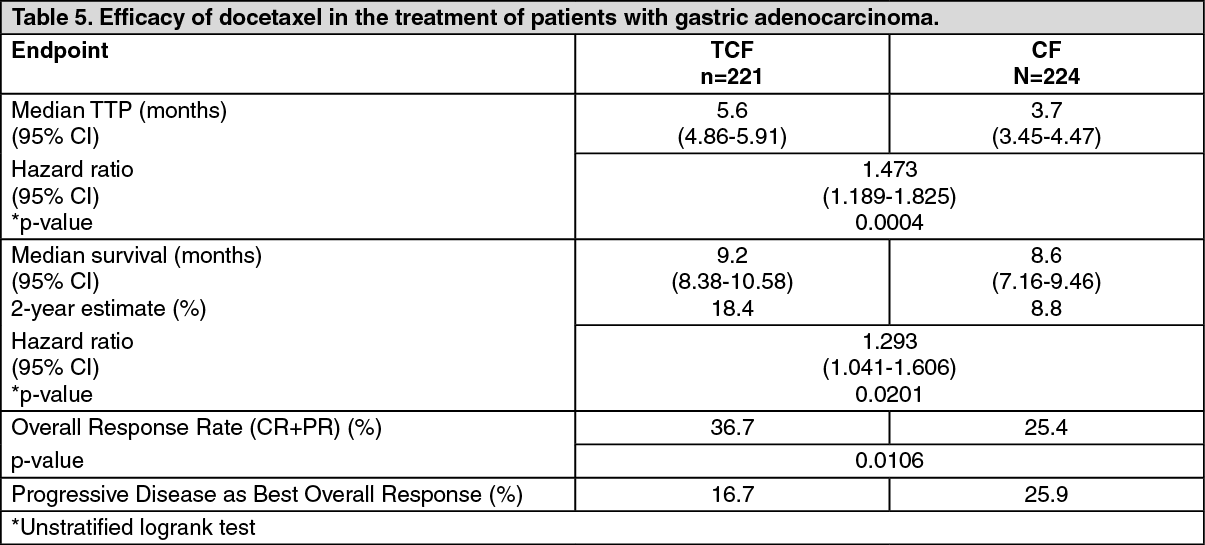
2 per day for 5 days). The length of a treatment cycle was 3 weeks for the TCF arm and 4 weeks for the CF arm. The median number of cycles administered per patient was 6 (with a range of 1-16) for the TCF arm compared to 4 (with a range of 1-12) for the CF arm. Time to progression (TTP) was the primary endpoint. The risk reduction of progression was 32.1% and was associated with a significantly longer TTP (p = 0.0004) in favor of the TCF arm. Overall survival was also significantly longer (p = 0.0201) in favor of the TCF arm with a risk reduction of mortality of 22.7%. Efficacy results are summarized in the following table: see Table 5.
Click on icon to see table/diagram/image
Subgroup analyses across age, gender and race consistently favored the TCF arm compared to the CF arm.
A survival update analysis conducted with a median follow-up time of 41.6 months no longer showed a statistically significant difference although always in favour of the TCF regimen and showed that the benefit of TCF over CF is clearly observed between 18 and 30 months of follow up.
Overall, quality of life (QoL) and clinical benefit results consistently indicated improvement in favor of the TCF arm. Patients treated with TCF had a longer time to 5% definitive deterioration of global health status on the QLQ-C30 questionnaire (p = 0.0121) and a longer time to definitive worsening of Karnofsky performance status (p = 0.0088) compared to patients treated with CF.
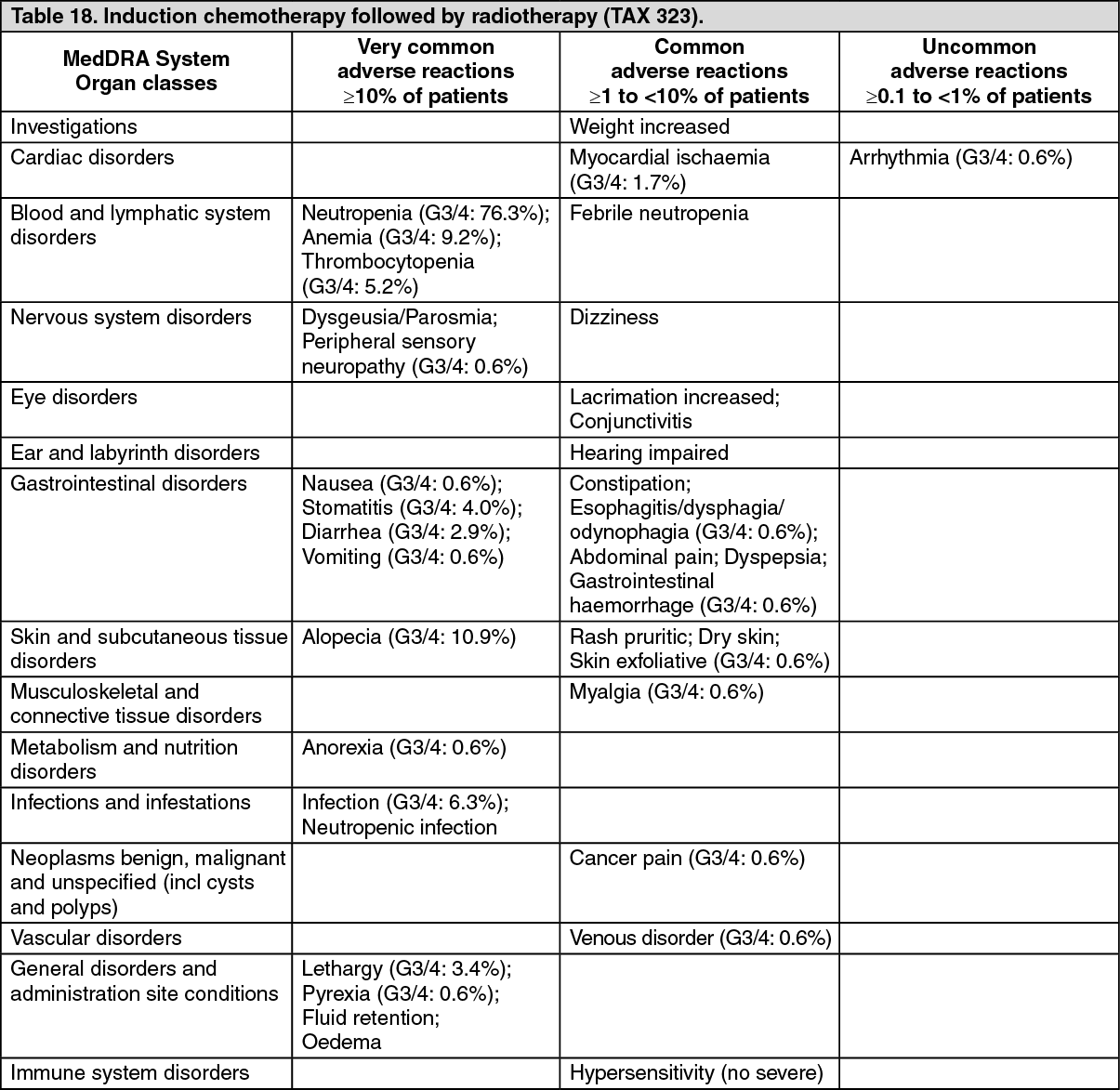
Head and neck cancer: Induction chemotherapy followed by radiotherapy (TAX323): The safety and efficacy of docetaxel in the induction treatment of patients with squamous cell carcinoma of the head and neck (SCCHN) was evaluated in a phase III, multicenter, open-label, randomized trial (TAX323). In this study, 358 patients with inoperable locally advanced SCCHN, and WHO performance status 0 or 1, were randomized to one of two treatment arms. Patients on the docetaxel arm received docetaxel (T) 75 mg/m
2 followed by cisplatin (P) 75 mg/m
2 followed by 5-fluorouracil (F) 750 mg/m
2 per day as a continuous infusion for 5 days. This regimen was administered every three weeks for 4 cycles in case at least a minor response (≥ 25% reduction in bidimensionally measured tumour size) was observed after 2 cycles. At the end of chemotherapy, with a minimal interval of 4 weeks and a maximal interval of 7 weeks, patients whose disease did not progress received radiotherapy (RT) according to institutional guidelines for 7 weeks (TPF/RT). Patients on the comparator arm received cisplatin (P) 100 mg/m
2 followed by 5-fluorouracil (F) 1000 mg/m
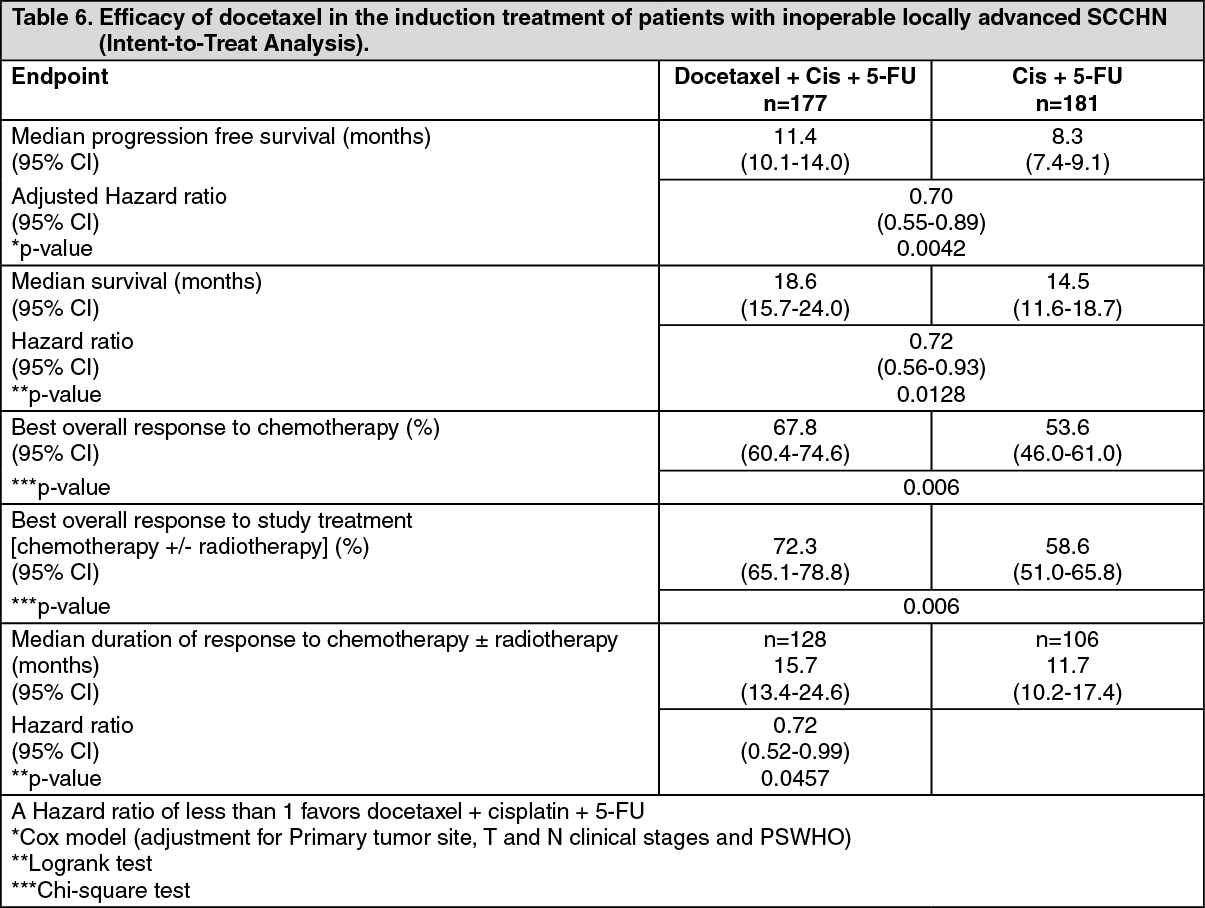
2 per day for 5 days. This regimen was administered every three weeks for 4 cycles in case at least a minor response (≥ 25% reduction in bidimensionally measured tumour size) was observed after 2 cycles. At the end of chemotherapy, with a minimal interval of 4 weeks and a maximal interval of 7 weeks, patients whose disease did not progress received radiotherapy (RT) according to institutional guidelines for 7 weeks (PF/RT). Locoregional therapy with radiation was delivered either with a conventional fraction (1.8 Gy - 2.0 Gy once a day, 5 days per week for a total dose of 66 to 70 Gy), or accelerated/hyperfractionated regimens of radiation therapy (twice a day, with a minimum interfraction interval of 6 hours, 5 days per week). A total of 70 Gy was recommended for accelerated regimens and 74 Gy for hyperfractionated schemes. Surgical resection was allowed following chemotherapy, before or after radiotherapy. Patients on the TPF arm received antibiotic prophylaxis with ciprofloxacin 500 mg orally twice daily for 10 days starting on day 5 of each cycle, or equivalent. The primary endpoint in this study, progression-free survival (PFS), was significantly longer in the TPF arm compared to the PF arm, p = 0.0042 (median PFS: 11.4 vs. 8.3 months respectively) with an overall median follow up time of 33.7 months. Median overall survival was also significantly longer in favor of the TPF arm compared to the PF arm (median OS: 18.6 vs. 14.5 months respectively) with a 28% risk reduction of mortality, p = 0.0128. Efficacy results are presented in the table as follows: see Table 6.
Click on icon to see table/diagram/image
Quality of life parameters: Patients treated with TPF experienced significantly less deterioration of their Global health score compared to those treated with PF (p = 0.01, using the EORTC QLQ-C30 scale).
Clinical benefit parameters: The performance status scale, for head and neck (PSS-HN) subscales designed to measure understandability of speech, ability to eat in public, and normalcy of diet, was significantly in favor of TPF as compared to PF.
Median time to first deterioration of WHO performance status was significantly longer in the TPF arm compared to PF. Pain intensity score improved during treatment in both groups indicating adequate pain management.
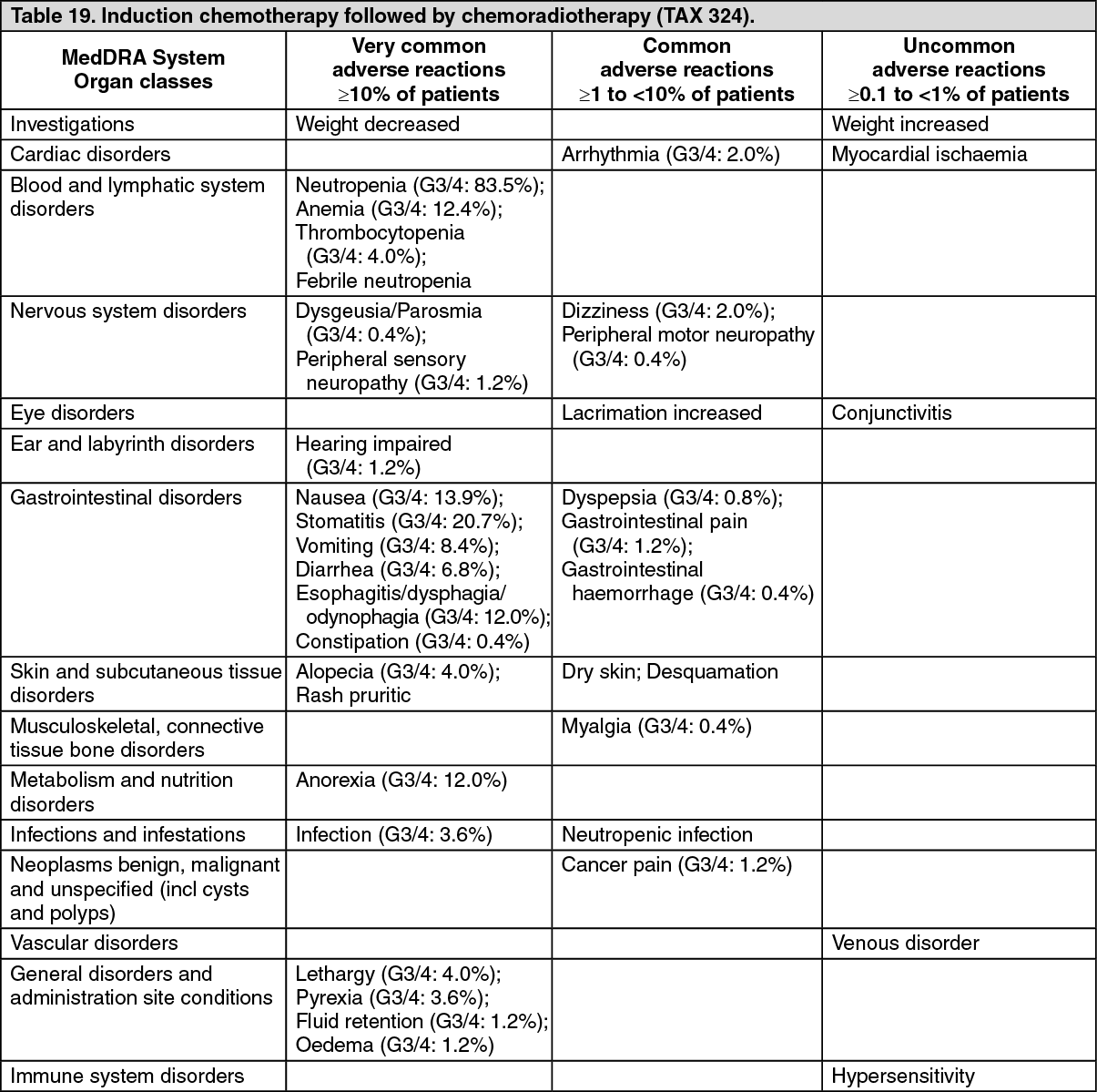
Induction chemotherapy followed by chemoradiotherapy (TAX324): The safety and efficacy of docetaxel in the induction treatment of patients with locally advanced squamous cell carcinoma of the head and neck (SCCHN) was evaluated in a randomized, multicenter open-label, phase III, trial (TAX324). In this study, 501 patients, with locally advanced SCCHN, and a WHO performance status of 0 or 1, were randomized to one of two arms. The study population comprised patients with technically unresectable disease, patients with low probability of surgical cure and patients aiming at organ preservation. The efficacy and safety evaluation solely addressed survival endpoints and the success of organ preservation was not formally addressed. Patients on the docetaxel arm received docetaxel (T) 75 mg/m
2 by intravenous infusion on day 1 followed by cisplatin (P) 100 mg/m
2 administered as a 30-minute to three-hour intravenous infusion, followed by the continuous intravenous infusion of 5-fluorouracil (F) 1000 mg/m
2/day from day 1 to day 4. The cycles were repeated every 3 weeks for 3 cycles. All patients who did not have progressive disease were to receive chemoradiotherapy (CRT) as per protocol (TPF/CRT). Patients on the comparator arm received cisplatin (P) 100 mg/m
2 as a 30-minute to three-hour intravenous infusion on day 1 followed by the continuous intravenous infusion of 5-fluorouracil (F) 1000 mg/m
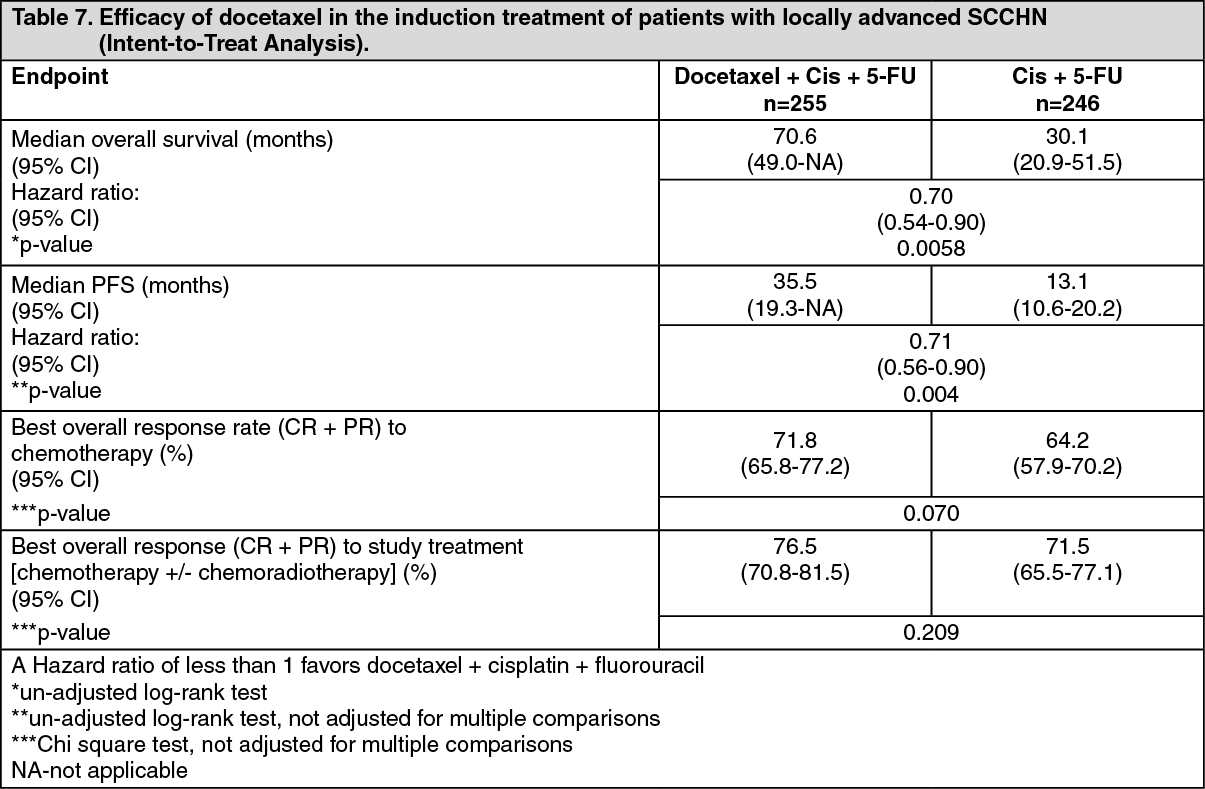
2/day from day 1 to day 5. The cycles were repeated every 3 weeks for 3 cycles. All patients who did not have progressive disease were to receive CRT as per protocol (PF/CRT). Patients in both treatment arms were to receive 7 weeks of CRT following induction chemotherapy with a minimum interval of 3 weeks and no later than 8 weeks after start of the last cycle (day 22 to day 56 of last cycle). During radiotherapy, carboplatin (AUC 1.5) was given weekly as a one-hour intravenous infusion for a maximum of 7 doses. Radiation was delivered with megavoltage equipment using once daily fractionation (2 Gy per day, 5 days per week for 7 weeks, for a total dose of 70-72 Gy). Surgery on the primary site of disease and/or neck could be considered at any time following completion of CRT. All patients on the docetaxel-containing arm of the study received prophylactic antibiotics. The primary efficacy endpoint in this study, overall survival (OS) was significantly longer (log-rank test, p = 0.0058) with the docetaxel-containing regimen compared to PF (median OS: 70.6 versus 30.1 months respectively), with a 30% risk reduction in mortality compared to PF (hazard ratio (HR) = 0.70, 95% confidence interval (CI) = 0.54-0.90) with an overall median follow up time of 41.9 months. The secondary endpoint, PFS, demonstrated a 29% risk reduction of progression or death and a 22 month improvement in median PFS (35.5 months for TPF and 13.1 for PF). This was also statistically significant with an HR of 0.71; 95% CI 0.56-0.90; log-rank test p = 0.004. Efficacy results are presented in the table as follows: see Table 7.
Click on icon to see table/diagram/image
Pharmacokinetics: The pharmacokinetics of docetaxel have been evaluated in cancer patients after administration of 20-115 mg/m
2 in phase I studies.
A population pharmacokinetic analysis has been performed with docetaxel in 577 patients. Pharmacokinetic parameters estimated by the model were very close to those estimated from phase I studies. The pharmacokinetics of docetaxel were not altered by the age or sex of the patient.
Absorption: Following the administration of a 100 mg/m
2 dose given as a one-hour infusion a mean peak plasma level of 3.7 μg/ml was obtained with a corresponding AUC of 4.6 h·μg/ml.
Distribution: The kinetic profile of docetaxel is dose independent and consistent with a three-compartment pharmacokinetic model with half lives for the, and phases of 4 min, 36 min and 11.1 h, respectively. The late phase is due, in part, to a relatively slow efflux of docetaxel from the peripheral compartment.
Docetaxel is more than 96% bound to plasma proteins.
Elimination: Mean values for total body clearance and steady-state volume of distribution were 21 l/h/m
2 and 113 l, respectively. Inter individual variation in total body clearance was approximately 50%.
A study of 14C-docetaxel has been conducted in three cancer patients. Docetaxel was eliminated in both the urine and faeces following cytochrome P450-mediated oxidative metabolism of the tert-butyl ester group, within seven days, the urinary and faecal excretion accounted for about 6% and 75% of the administered radioactivity, respectively. About 80% of the radioactivity recovered in faeces is excreted during the first 48 hours as one major inactive metabolite and 3 minor inactive metabolites and very low amounts of unchanged medicinal product.
In a small number of patients (n = 23) with clinical chemistry data suggestive of mild to moderate liver 1.5 times the ULN associated with alkaline function impairment (ALT, AST ≥ phosphatase ≥2.5 times the ULN), total clearance was lowered by 27% on average (see Dosage & Administration). Docetaxel clearance was not modified in patients with mild to moderate fluid retention and there are no data available in patients with severe fluid retention.
Pharmacokinetic interactions with other substances: When used in combination, docetaxel does not influence the clearance of doxorubicin and the plasma levels of doxorubicinol (a doxorubicin metabolite). The pharmacokinetics of docetaxel, doxorubicin and cyclophosphamide were not influenced by their coadministration.
Phase 1 study evaluating the effect of capecitabine on the pharmacokinetics of docetaxel and vice versa showed no effect by capecitabine on the pharmacokinetics of docetaxel (Cmax and AUC) and no effect by docetaxel on the pharmacokinetics of a relevant capecitabine metabolite 5'-DFUR.
Clearance of docetaxel in combination therapy with cisplatin was similar to that observed following monotherapy. The pharmacokinetic profile of cisplatin administered shortly after docetaxel infusion is similar to that observed with cisplatin alone.
The combined administration of docetaxel, cisplatin and 5-fluorouracil in 12 patients with solid tumors had no influence on the pharmacokinetics of each individual medicinal product.
The effect of prednisone on the pharmacokinetics of docetaxel administered with standard dexamethasone premedication has been studied in 42 patients. No effect of prednisone on the pharmacokinetics of docetaxel was observed.
Toxicology: Preclinical safety data: The carcinogenic potential of docetaxel has not been studied.
Docetaxel has been shown to be mutagenic in the
in vitro micronucleus and chromosome aberration test in CHO-K1 cells and in the
in vivo micronucleus test in the mouse. However, it did not induce mutagenicity in the Ames test or the CHO/HGPRT gene mutation assay. These results are consistent with the pharmacological activity of docetaxel.
Undesirable effects on the testis observed in rodent toxicity studies suggest that docetaxel may impair male fertility.



 Sign Out
Sign Out